thought leadership
Economic evaluation of vaccines: why is a QALY a recommended measure of benefit?
October 10, 2023
In the sixth of our series of updates examining market access for vaccines, Vanya Nikolova, Senior Consultant, shares why a quality-adjusted life-year (QALY) is a recommended measure of benefit in the economic evaluation of vaccines, and considers discounting of costs and health benefits in vaccine economic models across markets.
PRMA Consulting is now Avalere Health
Watch the full presentation
Demonstrating the value of vaccines: global NITAG and HTA requirements
On this slide you can see a summary of all the direct and indirect health outcomes that national immunization technical advisory groups (NITAGs) and health technology assessment (HTA) agencies expect to see reflected in vaccine economic appraisals. We have touched upon some of those already so we are not going to review all of them in detail.
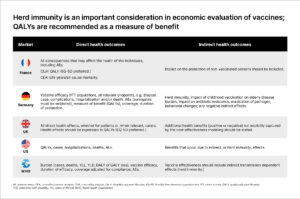
Quality-of life data are the basis of cost-utility analyses, with EQ-5D being the preferred utility instrument in France and the UK. Although market-specific utility data are generally preferred by decision-makers, quality of life evidence from other countries could also be used, provided that the data are sufficiently generalizable to the local setting.
In the case of infectious diseases in small children, the quality of life of parents is used as a proxy to measure the impact of the vaccination on the quality of life of children. However, recently some NITAGs have recognized that pediatric diseases have an impact on the quality of life of parents, and not only on the quality of life of the child. This has resulted in the “quality of life adjustment factor of 3” that was used in the meningitis B vaccine appraisal, where the QALY gain was multiplied by 3.
The types of costs that need to be reflected in the economic evaluation of vaccines depend on the perspective of the analysis
In France and Germany, both direct medical and non-medical costs need to be reflected in the economic evaluation. Medical costs include drug acquisition costs, costs associated with disease treatment, and the management of adverse events. Direct non-medical costs reflect expenses borne by the patient, their family, or caregivers such as costs of transportation to the hospital.
In contrast, in the UK and the US, only direct medical costs to the NHS or the healthcare provider need to be reflected in the economic analysis.
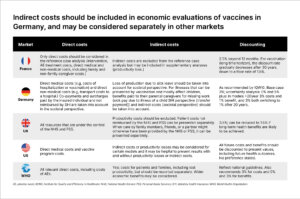
In addition to direct costs, vaccine economic models may also take into consideration indirect costs incurred due to loss of productivity or absenteeism from work as a result of the disease. These have been particularly impactful in the appraisal of infections that mostly affect children, such as meningitis, where parents need to take time off work to provide care.
However, NITAGs and HTA agencies in different countries have different expectations towards the inclusion of indirect costs in vaccine economic evaluations.
In the UK, indirect costs need to be excluded from the evaluation, whereas in France and Germany, these costs need to be incorporated in sensitivity analyses conducted from the societal perspective. In the US, indirect costs can be considered in the base case of some models; however, the Advisory Committee in Immunization Practices (ACIP) will expect to see a sensitivity analysis where indirect costs have not been excluded.
Discounting of costs in vaccine economic models varies across markets
Discounting of costs and health benefits is utilized in vaccine economic models, and recommended approaches and discount rates vary across markets.
- France: A constant discount rate of 2.5% should be applied. However, when the time horizon is very long the discount rate gradually decreases after 30 years, down to a floor rate of 1.5%.
- Germany: The Institute for Quality and Efficiency in Health Care (IQWiG) approach is adopted, where a constant 3% discount is applied in the base-case to all costs and benefits incurred after 12 months; however, inclusion of sensitivity analysis with constant discount rates of 0% and 5% is recommended. In models with a time horizon longer than 20 years, the Standing Committee on Vaccination (STIKO) recommends that the constant discount rate should be reduced from 3% to 1% after the 20-year mark.
- UK: The recommended discount rate in the UK is based on The National Institute for Health and Care Excellence (NICE) reference case for pharmaceuticals and is therefore set at 3.5%. However, when the Joint Committee on Vaccination and Immunisation (JCVI) appraised the human papillomavirus vaccine for boys, a 1.5% discount rate on health benefits and costs was applied due to the significant delay between immunization in adolescence and the onset of cancer approximately 50 years later.
- US: A specific discount rate has not been stipulated by ACIP although the economic modeling guidelines advise that all future costs and benefits should be discounted to present values.
Helping manufacturers establish the value of their vaccine with decision-makers
We will now look through a case study of how an assessment of NITAG and HTA vaccine evidence requirements can help manufacturers establish the value of their vaccine with decision-makers.
Watch the full presentation
Demonstrating the value of vaccines: global NITAG and HTA requirements